CBIC CIC - CBIC Certified Infection Control Exam
Which of the following blood-drawing methods is considered to be a needle-safe practice?
An infection preventionist has been asked to consult on disinfectant products for use in a long term care home. What should their primary concern be?
An infection preventionist (IP) is asked to participate on a team to decrease ventilator-associated pneumonia (VAP) rates in a 20-bed ICU. The IP provides the following information. What is the first quarter ventilator utilization ratio?
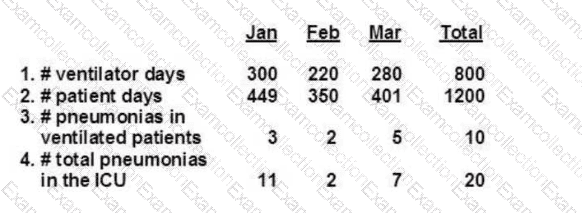
Data Provided (First Quarter):
Ventilator days (Jan–Mar total): 800
Patient days (Jan–Mar total): 1200
While completing compliance rounds in the Central Supply department, the infection preventionist notes items that have completed the sterilization process are showing evidence of moisture on the inside of the sterilization package. The FIRST step that the IP should take is to
Which statistical test is MOST appropriate for comparing infection rates before and after an intervention?
A task force formed to focus on Clostridioides difficile infections (CDIs). The topic of the meeting discussed selecting the correct germicidal wipe. What important factor does the infection preventionist review?
A 17-year-old presents to the Emergency Department with fever, stiff neck, and vomiting. A lumbar puncture is done. The Gram stain shows Gram negative diplocooci. Presumptive identification of the organism is
Based on the scenarios, when should an infection preventionist suspect an outbreak?
An infection preventionist is asked to recommend a product for disinfection of bronchoscopes. Which of the following agents would be appropriate?
The Sterile Processing Deportment alerts an infection preventionist that a load of surgical Instruments sterilized with high temperature steam:moist heat needs to be recalled. Which of the following Is the MOST likely reason for the recall?